- 50 Kitchen Design Ideas and Inspiration (2024)
- 25 Unique Kitchen Island Ideas and Design Inspiration
- Top 30 Kitchen Cabinet Hardware Ideas for Every Style
- 40 Kitchen Organization Ideas to Declutter Your Space
- 25 Covered Outdoor Kitchen Ideas for Your Backyard
- 40 Kitchen Storage Ideas for Small to Large Kitchens
- 25 Kitchen Remodel Ideas and Renovations for 2024
- 40 Modern Kitchen Ideas (Luxury Designs 2024)
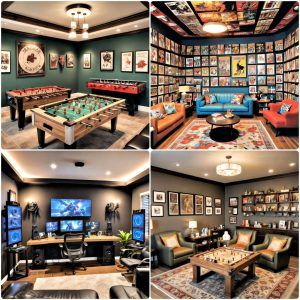
- 25 Cool Game Room Ideas for Every Gamer (2024)
- 25 Bathroom Remodel Ideas and Designs for 2024
- 25 Low Maintenance Side Yard Landscaping Ideas
- 25 Best Gravel Landscaping Ideas and Designs
- 25 Sloped Backyard Ideas on A Budget
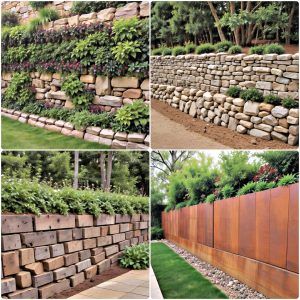
- 25 Retaining Wall Ideas for Stunning Landscaping Refresh
- 25 Rock Landscaping Ideas for Garden and Yard (2024)
- 25 Galley Kitchen Ideas and Designs on A Budget
- 25 Pool Cabana Ideas to Elevate Your Backyard (2024)
- DIY Kitchens Planner: 30 Ideas You Must Know (2024)
- 24 DIY Home Painting Tips You Must Know (2024)
- 30 Fence Decorating Ideas to Spruce Up Your Outdoor
- 25 Homemade DIY Jewelry Display Ideas
- 25 Easy DIY 4th of July Wreath Ideas
- 30 Paper Plate Crafts for Kids {Preschoolers & Toddlers}
- 25 Easy DIY Drawers: How To Make a Drawer
- 25 DIY Dollhouse Furniture Ideas Out Of Household Items
- 25 Free DIY Changing Table Plans Anyone Can Build
- 25 DIY Faux Fireplace Ideas: Build Your Own Fake Fireplace
- DIY Wood Countertops: 25 Ideas to Build Your Own
- 30 Easy DIY String Art Ideas and Crafts
- 20 Homemade DIY Welding Table Plans and Ideas
- 20 Homemade DIY Treadmill Desk Ideas
- 30 Easy DIY PVC Pipe Projects and Crafts
- 25 Homemade Lotion Recipes: How To Make Lotion
- 25 Cheap DIY Rain Barrel Ideas to Make and Save
- How to Make Ink: 20 Ways to Homemade Ink
- 30 DIY Keychain Ideas: Make Your Own Keychains
- 20 Homemade DIY Gun Rack Plans
- 20 Homemade DIY Tea Bags to Make Your Own
- 15 Ways to Hang a Door and Install a Door Frame
- 30 Free Friendship Bracelet Patterns: DIY Your Bracelets
- 25 Homemade Hand Scrub Recipes You Can Easily DIY
- 25 Easy DIY Epoxy Countertops: How To Step by Step
- 30 DIY Charging Station Ideas for Multiple Devices
- 20 Beautiful DIY Ladder Plant Stand Ideas
- 20 DIY Gas Fire Pit Ideas: How to Build Your Own
- 20 DIY Cloud Slime Recipes To Make at Home
- 15 Homemade Weed Killer Recipes You Can DIY
- 20 Free DIY Table Saw Fence Plans You Can Make
- 20 Homemade DIY Disc Golf Basket Ideas
- 20 Free DIY Subwoofer Box Plans to Build Your Own
- 20 Homemade DIY Flagpole Plans and Ideas
- 20 DIY Ballet Barre Ideas: Build Your Own Barre
- 25 Homemade DIY Dry Shampoo Recipes
- 30 Homemade DIY Foaming Hand Soap Recipes
- 50 Homemade DIY Body Scrub Recipes
- 35 Homemade DIY Lip Scrub Recipes to Make at Home
- 30 Homemade Deodorant Recipes You Can DIY
- 25 Homemade DIY Beard Oil Recipes to Make
- 15 DIY Professional Bath Bomb Recipe To Make
- 20 DIY Homemade Sunscreen Recipes You Can Make
- 25 Homemade DIY Shaving Cream Recipes
- 30 Homemade DIY Bath Bombs Recipes
- 80 DIY Homemade Soap Recipes – Make Your Own Soap
- 30 Easy Snowman Crafts and Ideas for Kids and Adults
- 25 Easy DIY Burlap Wreath Ideas to Make Your Own
- 30 Resin Crafts and DIY Projects to Make with Epoxy
- 25 DIY Water Fountain Ideas to Beautify Your Garden
- 30 Easy Popsicle Stick Crafts for All Ages
- 30 DIY Patio Furniture Plans and Ideas for Cozy Outdoor
- 30 Free DIY Entry Table Plans and Ideas
- 15 DIY Tablet Stand and iPad Stand Ideas
- 20 Clay Pot Painting and Decorating Ideas
- 25 Easy DIY Mail Organizer Ideas to Make
- 35 DIY Cutting Board Ideas and Free Plans
- 20 DIY Mason Jar Teacher Appreciation Gifts
- 30 Fun DIY Pineapple Crafts for Kids
- 25 Free DIY Beehive Plans to Build Your Own Bee Box
- 25 Free DIY Pantry Cabinet Plans to Build Your Own
- 30 New Years Eve Party Ideas to Celebrate In Style
- 30 Creative DIY Floor Lamp Ideas